

Introduction: Patients (pts) with MDS/MPN-RS-T have limited treatment options for anemia due to ineffective erythropoiesis. Luspatercept, the first-in-class erythroid maturation agent that enhances late-stage erythropoiesis, is approved by the FDA for treatment of anemia in adult pts with lower-risk (LR) MDS with ring sideroblasts (RS) or MDS/MPN-RS-T after erythroid-stimulating agent (ESA) failure. In the randomized, double-blind, phase 3 MEDALIST study, luspatercept significantly reduced transfusion burden vs placebo in pts with LR-MDS (NCT02631070; Fenaux P, et al. N Engl J Med 2020;382:140-51).
Here, we assess the efficacy and safety of luspatercept in pts with MDS/MPN-RS-T enrolled in the MEDALIST study.
Methods: Eligible pts were ≥ 18 years; had IPSS-R-defined Very low-, Low-, or Intermediate-risk MDS with RS; were refractory, intolerant, or unlikely to respond to ESAs (serum erythropoietin > 200 U/L); and required regular RBC transfusions. Pts were randomized 2:1 to luspatercept (1.0 mg/kg, titration to 1.75 mg/kg) or placebo administered subcutaneously every 3 wks. The primary endpoint was achievement of RBC transfusion independence (RBC-TI) ≥ 8 wks during Wks 1-24.
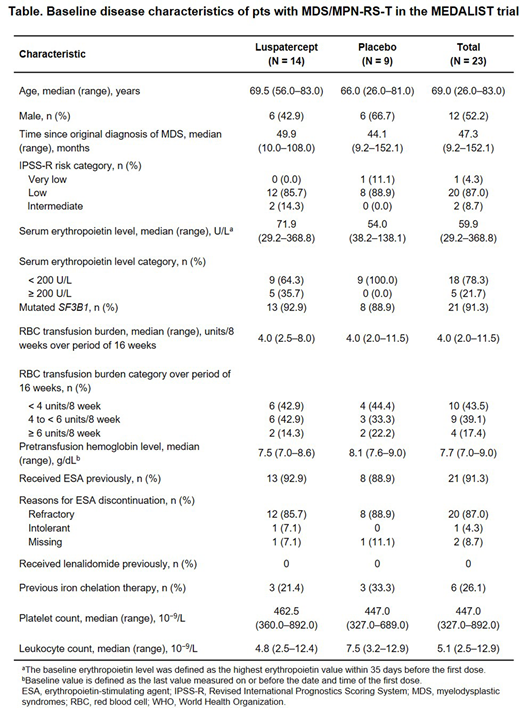
Results: A retrospective analysis identified 23/229 (10.0%) pts enrolled in the MEDALIST trial who had MDS/MPN-RS-T, per WHO 2016 criteria (Arber DA, et al. Blood 2016;127:2391-405); 14 received luspatercept and 9 received placebo. Pts in this subgroup received a median of 4.0 RBC units/8 wks (range 2.0-11.5) during the 16 wks prior to treatment. At baseline, pts had a median hemoglobin (Hb) level of 7.7 g/dL (range 7.0-9.0), a median leukocyte count of 5.1 × 109/L, a median platelet count of 447.0 × 109/L, and 18 (78.3%) pts had serum erythropoietin levels < 200 U/L (Table).
In the luspatercept arm, 9/14 (64.3%) pts with MDS/MPN-RS-T achieved the primary endpoint of RBC-TI for ≥ 8 wks during Wks 1-24, compared with 2/9 pts (22.2%) receiving placebo (odds ratio 11.3; 95% confidence interval [CI] 1.19, 106.12; P = 0.028).
Pts receiving luspatercept were significantly more likely to achieve clinical benefit (achieving RBC-TI ≥ 8 wks and/or modified hematologic improvement-erythroid [mHI-E] per IWG 2006 criteria [≥ 4 units/8 wks reduction in RBC transfusion in pts with ≥ 4 units/8 wks baseline RBC transfusion burden; Hb increase by ≥ 1.5 g/dL] during Wks 1-24 in pts with < 4 units/8 wks baseline RBC transfusion burden), compared with pts receiving placebo (78.6% vs 33.3%; P = 0.034). Median time from the start of clinical benefit response to end of treatment was 94.6 wks (range 8.0-150.0) in the luspatercept arm and 23.9 wks (range 23.7-57.9) in the placebo arm. During Wks 1-24, mHI-E was achieved by 10 luspatercept pts (6 were high transfusion burden [HTB; defined as baseline transfusion burden ≥ 4 units/8 wks] and 4 were low transfusion burden [LTB; defined as baseline transfusion burden < 4 units/8 wks]) and 1 placebo pt (1/5 HTB). RBC-TI ≥ 8 wks was achieved by 4/8 HTB pts receiving luspatercept (vs 0/5 placebo) and 5/6 LTB pts (vs 2/4 placebo).
After 24 wks, pts in the luspatercept arm had a mean Hb increase of +1.7 g/dL compared with an increase of +0.9 g/dL in pts in the placebo arm (least squares [LS] mean difference +0.85 g/dL; 95% CI −1.13, +2.82). Greater reductions from baseline in mean serum ferritin levels were seen with luspatercept (−121.8 μg/L) compared with placebo (−91.9 μg/L) over Wks 9-24 (LS mean difference −90.1; 95% CI −758.4, 578.2). Pts in the luspatercept arm had median platelet counts of 467.5 × 109/L and median leukocyte counts of 6.5 × 109/L post 24 wks of treatment, compared with pts in the placebo arm with 514.0 × 109/L and 6.2 × 109/L, respectively.
The incidence of specific TEAEs (occurring in ≥ 1 patient) are as follows: fatigue (1/14 [7.1%] luspatercept vs 1/9 [11.1%] placebo), dizziness (7/14 [50.0%] vs 0/9), dyspnea (3/14 [21.4%] vs 0/9), nausea (6/14 [42.9%] vs 2/9 [22.2%]), arthralgia (1/14 [7.1%] vs 0/9), diarrhea (6/14 [42.9%] vs 1/9 [11.1%]), and hypertension (3/14 [21.4%] vs 0/9). In the luspatercept arm, 1/14 (7.1%) pts experienced ≥ 1 thromboembolic event (transient ischemic attack) and 1/9 (11.1%) pts in the placebo arm progressed to AML (as of July 1, 2019).
Conclusions: Luspatercept demonstrated clinical efficacy in pts with MDS/MPN-RS-T with a generally well-tolerated safety profile. These data support the clinical benefits of luspatercept in this patient population with otherwise limited treatment options.
Komrokji:Geron: Honoraria; Novartis: Honoraria; Incyte: Honoraria; JAZZ: Honoraria, Speakers Bureau; AbbVie: Honoraria; Agios: Honoraria, Speakers Bureau; Acceleron: Honoraria; BMS: Honoraria, Speakers Bureau. Platzbecker:Janssen: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Honoraria; Geron: Consultancy, Honoraria; AbbVie: Consultancy, Honoraria; BMS: Consultancy, Honoraria; Novartis: Consultancy, Honoraria, Research Funding; Amgen: Honoraria, Research Funding. Fenaux:BMS: Honoraria, Research Funding; Abbvie: Honoraria, Research Funding; Novartis: Honoraria, Research Funding; Jazz: Honoraria, Research Funding. Garcia-Manero:Helsinn Therapeutics: Consultancy, Honoraria, Research Funding; AbbVie: Honoraria, Research Funding; Bristol-Myers Squibb: Consultancy, Research Funding; Amphivena Therapeutics: Research Funding; Jazz Pharmaceuticals: Consultancy; H3 Biomedicine: Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Acceleron Pharmaceuticals: Consultancy, Honoraria; Novartis: Research Funding; Genentech: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Onconova: Research Funding; Astex Pharmaceuticals: Consultancy, Honoraria, Research Funding; Merck: Research Funding. Mufti:Abbvie, Novartis: Consultancy; BMS, Novartis: Research Funding. Santini:Janssen: Research Funding; BMS, J&J, Novartis: Honoraria; Acceleron, BMS, Menarini, Novartis: Consultancy; Takeda, Pfizer: Membership on an entity's Board of Directors or advisory committees. Diez-Campelo:Takeda: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Celgene BMS: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau. Finelli:BMS: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Novartis: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Janssen: Membership on an entity's Board of Directors or advisory committees. Jurcic:AbbVie: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Syros Pharmaceuticals: Research Funding; Celgene: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; BMS: Consultancy, Research Funding; Daiichi-Sankyo: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees; Arog Pharmaceuticals: Research Funding; Astellas: Research Funding; Forma Therapeutics: Research Funding; Genentech: Research Funding; Kura Oncology: Research Funding; PTC Therapeutics: Research Funding. Greenberg:BMS: Research Funding; Aprea: Research Funding; Notable Labs: Research Funding; H3 Biotech: Research Funding. Sekeres:BMS: Consultancy, Membership on an entity's Board of Directors or advisory committees; Takeda/Millenium: Consultancy, Membership on an entity's Board of Directors or advisory committees; Pfizer: Consultancy, Membership on an entity's Board of Directors or advisory committees. Zeidan:Abbvie: Consultancy, Honoraria, Research Funding; Otsuka: Consultancy, Honoraria; Trovagene: Consultancy, Honoraria, Research Funding; Novartis: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Honoraria, Research Funding; Boehringer-Ingelheim: Consultancy, Honoraria, Research Funding; Leukemia and Lymphoma Society: Other; CCITLA: Other; Astex: Research Funding; MedImmune/Astrazeneca: Research Funding; Ionis: Consultancy, Honoraria; Epizyme: Consultancy, Honoraria; Aprea: Research Funding; ADC Therapeutics: Research Funding; Taiho: Consultancy, Honoraria; Seattle Genetics: Consultancy, Honoraria; Cardinal Health: Consultancy, Honoraria; Daiichi Sankyo: Consultancy, Honoraria; Astellas: Consultancy, Honoraria; Jazz: Consultancy, Honoraria; Cardiff Oncology: Consultancy, Honoraria, Other; Agios: Consultancy, Honoraria; BeyondSpring: Consultancy, Honoraria; Incyte: Consultancy, Honoraria, Research Funding; Acceleron: Consultancy, Honoraria; Celgene / BMS: Consultancy, Honoraria, Research Funding; Pfizer: Consultancy, Honoraria, Research Funding. DeZern:Astex: Research Funding; Celgene: Consultancy, Honoraria; MEI: Consultancy; Abbvie: Consultancy. Savona:Incyte: Consultancy, Research Funding; Sunesis: Consultancy, Research Funding; TG Therapeutics: Consultancy, Research Funding; BMS: Consultancy; AbbVie: Consultancy; Gilead: Consultancy; Karyopharm: Consultancy, Current equity holder in publicly-traded company; Ryvu: Consultancy; Boehringer Ingelheim: Patents & Royalties; Astex: Consultancy, Research Funding; Takeda: Consultancy, Research Funding. Shetty:BMS: Current Employment, Current equity holder in publicly-traded company. Ito:BMS: Current Employment, Current equity holder in publicly-traded company. Zhang:BMS: Current Employment. Ha:BMS: Current Employment. Sinsimer:BMS: Current Employment, Current equity holder in publicly-traded company. Backstrom:BMS: Current equity holder in publicly-traded company; Acceleron Pharma: Current Employment, Current equity holder in publicly-traded company. Verma:BMS: Consultancy, Research Funding; acceleron: Consultancy, Honoraria; Janssen: Research Funding; Medpacto: Research Funding; stelexis: Current equity holder in private company.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal